Abstract
Introduction.
Although rare, tsunamis have the potential to cause considerable loss of life and injury as well as widespread damage to the natural and built environments. The objectives of this review were to describe the impact of tsunamis on human populations in terms of mortality, injury, and displacement and, to the extent possible, identify risk factors associated with these outcomes. This is one of five reviews on the human impact of natural disasters.
Methods.
Data on the impact of tsunamis were compiled using two methods, a historical review from 1900 to mid 2009 of tsunami events from multiple databases and a systematic literature review to October 2012 of publications. Analysis included descriptive statistics and bivariate tests for associations between tsunami mortality and characteristics using STATA 11.
Findings.
There were 255,195 deaths (range 252,619-275,784) and 48,462 injuries (range 45,466-51,457) as a result of tsunamis from 1900 to 2009. The majority of deaths (89%) and injuries reported during this time period were attributed to a single event –the 2004 Indian Ocean tsunami. Findings from the systematic literature review indicate that the primary cause of tsunami-related mortality is drowning, and that females, children and the elderly are at increased mortality risk. The few studies that reported on tsunami-related injury suggest that males and young adults are at increased injury-risk.
Conclusions.
Early warning systems may help mitigate tsunami-related loss of life.
Funding Statement
This research was supported by the National Science Foundation’s Human and Social Dynamics Program (grant #0624106). The funding body played no role in the design, writing or decision to publish this manuscript.Introduction
A tsunami, the Japanese word for “large harbor wave,” is a series of large water waves produced by a sudden vertical displacement of water. Aquatic earthquakes are the most common cause, but volcanic activity, landslides and impacts of meteorites may also generate tsunamis. Earthquake-generated tsunamis develop when tectonic plates, either deep sea, continental shelf, or coastal, move abruptly in a vertical direction, and the overlying water is displaced. Waves created by these disturbances move in an outward direction, away from the source. In deep waters, the surface disturbance of water is relatively unnoticeable and may only be felt as a gentle wave. As the wave approaches shallow waters along the coast, it rises above the surface related to the amplitude of the underwater waves. The speed of the tsunami diminishes and the height of the wave increases as it reaches the shore line. The extent of inundation that occurs is largely dependent on local topography; in low lying areas flooding can be extensive and can reach far inland disrupting even non-coastal communities 1,2,3 .
While rare, high-impact tsunamis have the potential to cause widespread destruction and affect hundreds of thousands 4,5 . The 2004 Indian Ocean tsunami resulted in more than 225,000 deaths across twelve nations, and the 2011 Japan tsunami caused an estimated 28,000 deaths 6. Displacement and damage to infrastructure are also important contributors to the human, social, and economic effects of tsunamis 7. Few reviews of the impacts of tsunamis on human populations exist. Given the recent tsunami disasters in 2004 and 2009, a broader understanding of the characteristic effects of tsunamis on human populations could inform preparedness and response efforts. The objectives of this review were to describe the impact of tsunamis on the human population, in terms of mortality, injury, and displacement and to identify risk factors associated with these outcomes. This is one of five reviews on the human impact of natural disasters, the others being volcanoes, floods, cyclones, and earthquakes.
Methods
Data on the impact of tsunamis were compiled using two methods, a historical review of tsunami events and a systematic literature review for publications relating to the human impacts of tsunamis with a focus on mortality, injury, and displacement.
Historical Event Review
Data for the historical event review were obtained from two sources. The National Oceanic and Atmospheric Administration’s National Geophysical Data Center (NOAA-NGDC) tsunami database 8 consists of two sets of related files on tsunami events and a tsunami run-ups. The event file lists the cause (almost exclusively undersea earthquakes) that triggered tsunamis together with the total impact of a single event (i.e. the aggregate impact from multiple wave run-up locations together with the coordinates of the originating event). The run-up file includes wave characteristics and impacts in each affected location (multiple run-up reports per event). Records from the tsunami run-up file that met all of the following criteria were retained: 1) occurred between 1900 and 2009; 2) reported as definitely or probably occurring; 3) had a wave height ≥2.0m; and 4) resulted in ≥1 deaths. This yielded a total of 116 run-up reports from 82 different tsunami events.
The Centre for Research on the Epidemiology of Disasters’ Emergency Events (CRED EM-DAT) was the second data source used in the review. All wave/surge events that were reported between 1900 and 2009 in EM-DAT were included (n=58); data were initially exported in 2008 when CRED reported wave/surge events; this category was subsequently discontinued. For tsunami impacts reported by EM-DAT, zeroes were treated as missing values because they were used as placeholders and their inclusion in the analysis could contribute to the under estimation of tsunami impacts. The NOAA-NGDC run-up database was subsequently searched for events reported by EM-DAT that were previously excluded due to wave height <2.0m or uncertain reporting criteria, and NOAA-NGDC event data were added to the EM-DAT records. This process yielded a total of 151 records, including 58 events reported by EM-DAT and 134 run-ups reported by NOAA-NGDC. The run-up file was used to assess wave characteristics and outcomes. A separate event file comprised of 81 events was created by combining multiple reports of tsunami impact within a country into a single event. To create a summary record for each of event with multiple reports, human impacts at each location were summed, and the maximum wave height and inundation depth were applied. The event file had 94 events, including 58 reported by EM-DAT and 71 by NOAA, and was used to assess frequency and distribution of tsunamis and their impact by country. Findings presented in this review are based on the 151 run up file. Both run-up and source data can be accessed online at https://www.jhsph.edu/refugee/natural_disasters/_Event_Tsunamis.html.
In order to examine country- and event-specific characteristics associated with low and high levels of tsunami mortality, deaths were categorized as follows: low (<10 deaths), medium (11-75 deaths) and high (>75 deaths). Bivariate tests for associations between tsunami mortality and the following characteristics were performed using χ2 (categorical measures) and ANOVA (continuous measures): time period (dichotomized, 1900-1955 and 1956-2009), region as defined by the World Health Organization (WHO), income level (World Bank), gross domestic product (GDP), GINI (measure of income inequality), distance from source (quartiles), wave height (dichotomized, <6.65 and >6.65) and earthquake magnitude. For the region variable, only three events were reported in Africa and because all were related to the 2004 Indian Ocean tsunami, they were grouped with Southeast Asian; only one event was recorded in the Eastern Mediterranean region which was grouped Europe .All analyses were performed using Stata Statistical Software, Version 11.0 9
Systematic Literature Review
Key word searches in MEDLINE (Ovid Technologies, humans), EMBASE (Elsevier, B.V., humans), SCOPUS (Elsevier B.V., humans), and Web of Knowledge, Web of Science (Thomson Reuters) were performed to identify articles published in July 2007 or earlier that described natural hazards and their impact on human populations. Key words used to search for natural hazards included natural hazard(s), natural disaster(s), volcano(es), volcanic, volcanic eruption, seismic event, earthquake(s), cyclone(s), typhoon(s), hurricane(s), tropical storm(s), flood(s), flooding, mudslide(s), tsunami(s), and tidal wave(s). Key words included for impact on human populations were affected, damage(d), injury, injuries, injured, displaced, displacement, refugees, homeless, wounded, wound(s), death(s), mortality, casualty, casualties, killed, died, fatality, fatalities and had to be used in either the title, abstract or as a subject heading/key word. The search resulted in 2,747 articles from MEDLINE, 3,763 articles from EMBASE, 5,219 articles from SCOPUS, and 2,285 articles from ISI Web of Knowledge. Results from the four databases were combined and duplicates were excluded to yield a total of 9,958 articles. . One search was done for all the five natural hazards described in this set of papers. This paper describes the results for tsunamis. The systematic review is reported according to the PRISMA guidelines.
Title screening was performed to identify articles that were unrelated to natural disasters or human populations. Each title was screened by two independent reviewers and was retained if either or both reviewers established that inclusion criteria were met. To ensure consistent interpretation of inclusion criteria, percent agreement was assessed across reviewers for a small sample of articles, and title screening began after 80% agreement on inclusion was achieved. A total of 4,873 articles were retained for abstract review. Articles that met one or more of the following criteria were excluded in the abstract screening: language other than English; editorial or opinion letter without research-based findings; related to environmental vulnerability or hazard impact but not human populations; individual case report/study; focus on impact/perceptions of responders; and not related to human or environmental vulnerabilities or impacts of hazards. As with the title screening, overall percent agreement between reviewers was assessed, and abstract screening began after achieving 80% agreement. Each abstract was screened by two independent reviewers and was retained if either or both reviewers established that inclusion criteria were met. During the abstract review, included abstracts were coded for event type, timeframe, region, subject of focus, and vulnerable population focus.
A total of 126 articles were retained for full article review. Articles discussing the impacts of natural disasters on human populations in terms of mortality, injury, and displacement were prioritized for review. A total of 64 articles on tsunamis meeting the aforementioned subject focus criteria were retained for full review. Upon full review, 27 articles were retained including 23 that underwent dual review and standardized data abstraction, two identified as review articles 10,11, one policy article 12 and one article on mitigation 13 (Figure 1). Following the systematic review, a hand search was conducted using the databases and key words listed above to identify relevant articles published between July 2007 when the initial search was conducted and October 2012; seven additional articles were identified that met criteria for full review. In total, 34 articles relating to risk factors for mortality, injury or displacement were identified; summaries of articles with primary data (n=30) are presented in Table 1.

Fig. 1: Overview of the systematic literature review process for tsunamis
* Displacement is excluded from the table because no primary data on displacement was collected in only three studies: MMWR, 2006; Rofi, 2006; and Yamada, 2006; ** Additional articles from the hand search through October 2012
Article
Event
Summary
Mortality (n=14)
Injury & Morbidity (n=19)
Tsuji et al., 199515
June 3, 1994, East Java, Indonesia
Field survey to assess the destruction of the tsunami
223 deaths reported
Neither reported
Tsuji et al., 199516
December 12, 1992, Flores Island
Field survey to assess the destruction of the tsunami
1690 deaths reported
Neither reported
Davies et al., 200317
July 17, 1998, Aitape, Papua New Guinea , 1998
Interviews and field investigations to describe the physical characteristics of tsunamis.
1600 deaths reported; primary causes of death were drowning and impacts with hard objects
Neither reported
Brennan and Rimba., 200518
December 26, 2004, Indonesia
Rapid health assessment to determine the public health impact of the tsunami in three communities of the Aceh Jaya district
70% of the population died
Injury data not reported85% of children <5 yrs old experienced an illness
Calder & Mannion, 200519
December 26, 2004, Sri Lanka
Review of findings from a DFID needs assessment with an emphasis on trauma/ orthopedic and psychiatric services
Not reported
100 injuries reportedNo morbidity data reported
Johnson & Travis, 200520
December 26, 2004, Thailand
Facility-based, retrospective record review to describe tsunami-related injuries at the provincial hospital in Krabi province.
25 deaths reported
1357 injuries reportedNo morbidity data reported
Lee et al., 200521
December 26, 2004, Indonesia
Description of primary health care services delivered in an internally displaced persons camp by a medical team from Singapore
Not reported
1958 people injuredNo morbidity data reported
Lim et al., 200522
December 26, 2004, Sri Lanka
A description of the patients treated by two Korean medical teams over a nine day period following the tsunami
Not reported
4710 injuries reported; primary causes were running from the tsunami and surviving in wreckageNo morbidity data reported
Maegele et al., 200523
December 26, 2004, Thailand
Observational study of patients seen at an adult intensive care unit a university hospital
Not reported
17 injuries reported; the primary cause of injury was due to hitting floating debrisNo morbidity data reported
Chambers et al., 200624
December 26, 2004, Indonesia
Description of surgical and humanitarian assistance operations of a joint Australian and New Zealand operation in the four week period following the tsunami
Not reported
71 injuries reportedNo morbidity data reported
Fan, 200625
December 26, 2004, Indonesia
Description of patients treated in Banda Aceh by a medical team from Singapore in the first few weeks following the Tsunami
Not reported
2183 injuries reported; primary causes was being caught in the wave and struck by debris. No morbidity data reported
Kwak et al., 200626
December 26, 2004, Sri Lanka
Descriptive study of patients treated by Korean surgical and medical personnel from January 2 to 8, 2005
Not reported
2807 individuals treated for medical problems (82%) and injuries (18%)
MMWR, 200627
December 26, 2004, Indonesia
Three household surveys to assess affected populations and evaluate effectiveness of relief interventions 7 months post-disaster
Not reported
Neither reported
Nishikiori et al., 200628
December 26, 2004, Sri Lanka
Household survey to assess mortality among the internally displaced population
446 deaths reported
Neither reported
Nishikiori et al., 200629
December 26, 2004, Sri Lanka
Household survey to assess mortality among the internally displaced population
446 deaths reported; primary cause of death was drowning
Neither reported
Redwood –Campbell & Riddez, 200630
December 26, 2004, Indonesia
Descriptive study of outpatients at an International Committee of the Red Cross hospital nine weeks following the tsunami
Not reported
271 injuries reported
Rodriguez et al., 200631
December 26, 2004, India and Sri Lanka
Observations and key-informant interviews to describe the societal impacts of the disaster
250000 deaths reported; primary cause for death was drowning
Neither reported
Rofi, et al., 200632
December 26, 2004, Indonesia
Household survey to estimate mortality and displacement
295 deaths reported
Neither reported
Roy, 200633
December 26, 2004, India
Descriptive study of deaths and individuals treated at a secondary care hospital in the days following the tsunami
62 deaths reported; primary cause of death was drowning
Minor injuries reported 17% of patients showed symptoms of PTSD
van Griensven et al., 200634
December 26, 2004, Thailand
Multi-stage, cluster survey to assess the mental health of displaced and non-displaced populations following the tsunami
Not reported
Injury data not reported1061 mental health issues reported; primary cause due to tsunami
Yamada et al., 200635
December 26, 2004, Sri Lanka
Needs assessment conducted to understand tsunami impact on specific population groups and on the health care system
Not reported
Injury data not reportedGeneral mental health consequences of the disaster reported
Doocy et al., 200736
December 26, 2004, Indonesia
Estimation of tsunami mortality using GIS-based vulnerability modeling
131066 deaths estimated
Neither reported
Doocy et al., 200737
December 26, 2004, Indonesia
Four two-stage cluster household surveys to assess mortality and associated risk factors
1642 deaths reported
Neither reported
Johnson & Travis, 200638**
December 26, 2004, Thailand
A description of individuals treated at a provincial tertiary hospital in the weeklong period following the event
Not reported
1357 injuries reported
Johnson & Travis, 200639**
December 26, 2004, Thailand
Application of the tri-modal death model to mortality and injury post-tsunami
Not reported
Not reported
Meynard et al., 200840**
December 26, 2004, Indonesia
Cluster survey s to assess health of children affected by the disaster
Not reported
Injury data not reported7-13% malnourished and 68% experienced sickness
Prasartritha et al., 200841**
December 26, 2004, Thailand
Retrospective record review of injury care seekers at three hospitals
Not reported
2311 injuries reportedMorbidity data not reported
Doocy et al., 200942**
December 26, 2004, Indonesia
Three two-stage cluster household surveys to assess injury and associated risk factors
17.7% (CI:16.8-18.6) of the population died
707 injured individualsMorbidity data not reported
Doung-ngern et al., 200943**
December 26, 2004, Indonesia
Assessment of wound treatment among care seekers at four public hospitals
Not reported
513 injuries (wounds) reportedMorbidity data not reported
Nagamatsu et al, 201244**
March 11, 2011 Japan
Review of DMAT response
282 deaths from deteriorating pre-existing chronic medical conditions
4891 injured patients at the Ishinomaki Red Cross Hospital
Results
Historical Event Review
Between 1900 and 2009, 94 tsunamis that affected human populations were recorded. The frequency of events was relatively constant through the 1980s, after which a dramatic increase was reported (Figure 2). This increase is likely the result of improvements to monitoring and reporting systems. Tsunami frequency and mortality were concentrated in the Western Pacific, Southeast Asia, and Americas regions, each of which accounted for almost one third of tsunami events and deaths, but Southeast Asia accounted for 52% of the tsunami-affected population from 1900 – 2009 and 95% of the tsunami affected population from 1980 – 2009 (Figure 4). An estimated 2.5 million people were affected by tsunamis between 1900 and 2009. A sharp increase in tsunami mortality and affected populations was observed from 2000 to 2009 as a result of the 2004 Indian Ocean tsunami (Figure 3). The overall impact of tsunamis on human populations is summarized in Table 2.
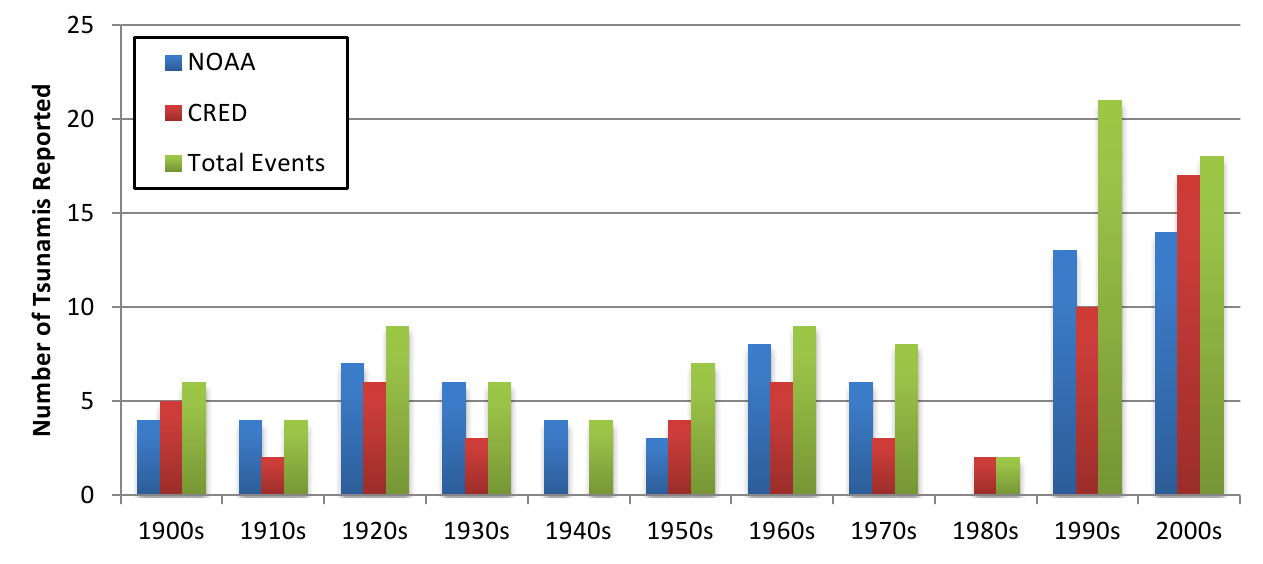
Fig. 2: Reporting of tsunamis by source and decade

Fig. 3: Tsunami events affecting human populations by decade
*Regions as defined by the World Health Organization
Fig. 4: Tsunamis and their impact on human populations by region, 1980-2009*
Notes: figures based on the highest reported number of deaths or injuries in an event in one country. Homeless and total affected populations are reported only by EM-DAT, thus ranges are not presented for overall impact estimates.
Cumulative Impact of Tsunamis, 1900-2009 [1970-2009]
Human Consequence
# of Events
Best Estimate
Range
1900-2009 (n=94)
1980-2009 (n=16)
1900-2009 (n=94)
1980-2009 (n=16)
1900-2009 (n=94)
1980-2009(n=16)
Deaths
87
16
255,195
230,012
252,619-275,784
228,932 – 231,091
Injuries
22
9
48,462
14,029
45,466-51,457
11,033 – 17,024
Homeless
12
7
1,081,764
1,034,214
—
—
Total Affected
25
4
2,532,189
2,479,689
—
—
Event Summary Statistics
Human Consequence
# of Events
Median
Mean
Range
1900-2009 (n=94)
1980-2009 (n=16)
1900 – 2009 (n=94)
1980-2009 (n=16)
1900-2009 (n=94)
1980-2009 (n=16)
1900-2009 (n=94)
1980-2009 (n=16)
Events with deaths
87 [92.5%]
16 [100%]
50
2,963
14,839
1-165,708
1-165,708
Reported by EM-DAT
53 [56.4%]
16 [100%]
64
91
4,559
14,339
1-165,708
1-165,708
Reported by NOAA
69 [73.4%]
15 [93.75%]
61
108
3,623
15,375
1-165,659
1-165,659
Events with Injuries
22 [23.4%]
9 [56.25%]
218
2,878
2,339
5,255
2-23,176
2-23,176
EM-DAT
13 [13.8%]
9 [56.25%]
543
2,214
3,320
5,113
2-23,176
2-23,176
NOAA
10 [10.5%]
10 [6.25%]
127
6,534
885
6,534
7-6,534
—
Homeless, all events
12 [12.8%]
12 [43.75%]
4773
4,296
90,147
147,745
70-532,898
70-532,898
Total Affected, all events
25 [26.6%]
25 [87.5%]
5063
21,457
101,288
177,745
2-1,109,306
194-1,109,306
Tsunami Characteristics. The physical characteristics of tsunamis were reported by NOAA-NGDC and included distance of the tsunami run-up from source, wave height, and earthquake magnitude. The median distance from source was 119 km (mean 810 km; range 7-10,621 km), and the median wave height was 6.7m (mean 13.0m; range 1.8 -67.1m). The majority of the tsunamis reported were due to earthquakes (95.5%), with small minorities resulting from landslides (3.0%), volcanoes (0.8%), and meteorological events (0.8%). Median magnitude for earthquake generated tsunamis was 8.1 (mean 8.1; range 6.3-9.5).
Mortality. Deaths were reported in 92.6% (n=94) of tsunamis occurring between 1900 and 2009. There were an estimated 255,195 deaths (range 252,619-275,784) resulting from tsunamis recorded in the historic event review, with the 2004 Indian Ocean tsunami accounting for an estimated 227,497 deaths (89%) of all mortality. Deaths were concentrated in Indonesia (62% or 170,689 deaths), Sri Lanka (13% or 35,399 deaths), Thailand (3.2%, 8,876 deaths) and the Philippines (3% or 8,137 deaths). Apart from rare high-impact events such as the 2004 Indian Ocean tsunami, mortality levels in tsunamis tend to be relatively low with a median of 50 deaths per event (mean=2,963,range 0-165,708) when using the highest reported death toll.
Table 3 presents results of the bivariate analyses between tsunami characteristics and mortality. Time period, and GINI coefficient were not statistically associated with tsunami mortality. There were considerable differences in mortality levels by WHO region, with the majority of tsunami events that occurred in the Americas resulting in low (<10) deaths and 50% of events in the South East Asian region resulting in high (>75) deaths (p<.001). Both World Bank-defined income level and per capita GDP were significantly associated with tsunami mortality. Whereas the majority of events in high income countries resulted in ten or fewer deaths, a considerably greater number of events in low and lower-middle income countries resulted in greater than ten deaths (p=.009). Similarly, events that resulted in greater than 75 deaths occurred in countries or territories with per capita GDPs that were more than two times lower than countries that experienced fewer tsunami deaths (p<.001). While the data show an inverse associations between tsunami mortality and distance from source (p=.001) and a positive association between mortality and wave height (p=.016), it is important to note that information pertaining to both measures were missing in a considerable proportion of events, particularly those occurring earlier in the study period.
Characteristic
<=10 deaths
(n = 57)11-75 deaths
(n = 51)>75 deaths
(n = 44)P-value
Time period, n (%)
1900-1955
26 (41)
22 (35)
15 (24)
.485
1956-2009
31 (35)
29 (33)
29 (33)
WHO Region, n (%)
Americas
36 (63)
12 (21)
9 (16)
<.001
Western Pacific
8 (21)
19 (50)
11 (29)
Southeast Asia & Africa
8 (20)
12 (30)
20 (50)
Europe & Eastern Mediterranean
5 (29)
8 (47)
4 (24)
World Bank Development Level, n (%)
Low income
6 (38)
6 (38)
4 (25)
.009
Lower-middle income
10 (20)
17 (35)
22 (45)
Upper-middle income
4 (25)
6 (38)
6 (38)
High Income
37 (52)
22 (31)
12 (17)
Distance from Source (km), n (%)
< 67
7 (25)
14 (50)
7 (25)
.001
68 – 119
11 (41)
8 (30)
8 (30)
120 – 468
12 (44)
7 (26)
8 (30)
Greater than 468 km
19 (70)
6 (21)
2 (7)
Distance missing
8 (19)
16 (37)
19 (44)
Wave Height (m), n (%)
< 6.65
31 (53)
18 (31)
10 (17)
.016
> 6.65
19 (32)
20 (34)
20 (34)
Missing wave height
7 (21)
13 (38)
14 (41)
Per capita GDP (USD), mean (SD)
29368 (2605)
20561 (3104)
12584 (2364)
<.001
Earthquake Magnitude, mean (SD)
8.12 (0.11)
8.06 (0.14)
8.18 (0.12)
.784
GINI Coefficient, mean (SD)
40.28 (0.77)
37.72 (1.12)
38.82 (1.27)
.209
Injury. Injury reports were only available in 22 (23.4%) events for a total of 48,462 injuries (range 45,466-51,457). A typical tsunami caused 218 injuries (median value) but the distribution was skewed by rare large-scale events (mean injured=2,339, range=0-23,176). To more accurately estimate the total number of injuries due to tsunamis, it was presumed that injuries would occur in events where deaths were reported. There were 87 tsunami events with fatalities; when the median and mean for injuries were applied to the remaining 65 events with fatalities, it was estimated that between 14,170 and 152,035 unreported tsunami-related injuries occurred worldwide between 1900 and 2009.
Systematic Literature Review
Mortality. Of the 33 articles reviewed, 12 reported on mortality, including mortality counts or rates and/or risk factors for death (Table 4). Age and sex were described as risk factors for death in three articles, all from the 2004 Indian Ocean tsunami 28,32,37. In both Indonesia and Sri Lanka, significantly higher death rates were reported among females who were 1.4 to 2.1 times more likely to perish than males. Significantly elevated risk of death was also observed in children (1.8 to 4.3 times) and older adults (2.1 to 3.1 times) who were more likely to die compared with younger/middle age adults. Other risk factors included education which was inversely associated with mortality risk 28; fisheries-based livelihoods 28,32indoor location at the time of the tsunami and home destruction 28 and the physical environment 15. The majority of tsunami deaths were due to drowning 11,14.
Article
Country
Mortality
Sex as a risk factor
Age as a risk
N
Rate
Tsuji et al., 199515
Indonesia
223
6.9% (Lampon); 3.9% (Rajekwesi & Pancer)
Not reported
Not reported
Tsuji et al., 199516
Flores Island
1,690
Not reported
Not reported
Not reported
Davies et al, 200317
Papua New Guinea
1,600
Not reported
Not reported
Not reported
Brennan, 200518
Indonesia
~5,460-6,090
70% (Calang)
Not reported
Not reported
Johnson et al, 200520
Thailand
25
Not reported
Not reported
Not reported
Nishikiori et al., 200628
Sri Lanka
457
12.6%
Higher mortality was observed among females at 17.5% vs. 8.2% for males.
Elevated mortality among children (<5yrs: 31.8% and 5-9 yrs: 23.7%) and the elderly (15.3%) as compared to 7.4% for adults 20-29 yrs.
Nishikiori et al., 200629
Sri Lanka
446
0.25 deaths / 10,000 population
Not reported
Not reported
Rodriguez et al., 200631
India and Sri Lanka
250,000
Not reported
Not reported
Not reported
Rofi, et al., 200632
Indonesia
295
13.9% (CI:12.4-15.4)
Risk of mortality was 1.9 (CI:1.5-3.0) times greater in females than males.
Elevated risk of death for children <10yrs (2.3, CI: 1.6-3.4) and adults >60yrs (3.1, CI: 1.9-4.9) as compared to 20-39 yr olds.
Roy, 200633
India
62
0.85 deaths / 10,000 population
Not reported
Not reported
Doocy et al, 200736
Indonesia
131,066
Modeled rates of 23.7% (exposed population)
Not reported
Not reported
Doocy et al, 200737
Indonesia
1,642
16.3% (crude) and 14.1% (adjusted)
Higher mortality rate in females (16.4%) than males (12.0%). Risk for death was 1.4 (CI: 1.3-1.6) times greater in females.
Elevated mortality among children (<0-yrs: 19.8%) and older adults (60-69yrs: 22.6%, 70+yrs: 28.1%) (15.3%) as compared to 10.8% among 20-39yr olds.
Injury. Tsunami-related injuries were reported in 18 articles though only ten provided detailed information on injury types or risk factors (Table 5). Only one study estimated a population-based injury rate of 8.5% in Indonesia following the 2004 tsunami 42. Other articles described the proportion of care seekers with tsunami-related injuries or included only patients with tsunami-related injuries, preventing comparisons in injury patterns across events and locations. Only two studies described risk factors for tsunami-related injury, both with similar findings, in the 2004 Asian tsunami. The first, a study of patients seen by a medical team in Sri Lanka, observed that males and adults (15-64 years) seeking care for injuries were over-represented, suggesting these population sub-groups had higher injury rates 26. The second used household survey data from Indonesia and reported lower injury risk among females (OR=0.81) and the highest injury rates among those 20-49 years of age. The risk factors for injury were opposite those of mortality suggesting that those more likely to survive the tsunami were also more likely to be injured 42. The most common types of injuries were wounds due to physical impact with debris, fractures, and near drowning and/or aspiration 21,22,23,25,26,30,42 . As compared to other types of natural disasters, tsunamis often result in relatively high mortality but have lower rates of injury 11.
Article
Country Affected
Injuries Reported
Injury Type
Notes
# injured / cases
Injury Rate
Respiratory Injury or Near Drowning
Musculo-skeletal or Orthopedic Injury
Traumatic Injury / Wound
Dermatologic Injury
Gastro-intestinal Injury
Other
Calder et al, 200519
Sri Lanka
100
Not reported
Open fractures repair, wound debridement and skeletal traction were the most common procedures
Lee et al, 200521
Indonesia
1958
Not reported
27%
72%
Lim et al, 200522
Sri Lanka
4710
Not reported
28%
29%
34% of cases were non- tsunami related chronic conditions
Maegele et al, 200523
Thailand
17
Not reported
Closed fracture 35%; open fracture 24%
Soft tissue hip/ lower extremity 88%; soft tissue upper extremity 29%
Head injuries 18%, hemopnueu-mothorax 18%, thoracic trauma 14%
Johnson et al, 200540
Thailand
1357
Not reported
n=31 (2%)
n=33 (2%)
n=65 (5%)
Head, n=18 (1%); abdominal n=12 (1%), chest/ thoracic (n=3, 0%)
Retrospective study of facility data. Reports on injuries and evolution of pathology.
Chambers et al, 200624
Indonesia
71
Not reported
9% fracture management
34% wound debridement
24% changing dressing under anesthetic
Reports on surgical procedures only; 69% were for tsunami-related injuries.
Fan, 200625
Indonesia
1021
Not reported
32%
11% musculo-skeletal
25%
10%
10%
2% neurologic injuries
Kwak, 200626
Sri Lanka
2807
Not reported
33%
22% orthopedic
8%
13%
4%
4% headache
Adults and males had higher injury rates
Redwood –Campbell et al, 200630
Indonesia
271
12% of cases were tsunami related
Most tsunami related injuries were fractures, wounds, and aspiration pneumonia.
Doocy et al, 200942
Indonesia
707
8.5% (CI: 7.9-9.2)
4%
8% fractures
75%
13% other (unspecified)
Lower injury risk among females (OR=0.81, CI 0.61-0.96); highest injury rate among 20-49yr age group
Discussion
Main Findings
From 1900 to 2009, approximately 2.5 million people were affected by tsunamis including over 255,000 deaths and an estimated 50,000 injuries. The mortality and population affected estimates presented in this study are consistent with other reviews of global tsunami events 11 It is likely that the number injured is underestimated, given the low frequency with which this figure was reported, particularly in the first half of the 20th century. When the mean and median numbers injured were applied to events that resulted in deaths it was estimated that between 10,900 and 116,950 unreported tsunami-related injuries occurred worldwide during this time period. It is important to note, that studies have shown that that ratio of deaths to injuries following a tsunami is typically significantly higher compared with other natural disaster types 11.
This study is the first to examine the influence of place and event characteristics on tsunami mortality. Analyses of tsunami run-up data from 1900 to 2009 reveal that events occurring in the South East Asian region were significantly more likely to result in greater numbers of deaths compared to other regions, and this finding persisted even after excluding the 2004 Indian Ocean tsunami. Examination of the relationship between mortality levels and the two poverty measures (World Bank income level and per capita GDP) demonstrate that risk of mortality event is significantly higher in low-income countries. Lastly, certain event characteristics are more likely to be predictive of mortality than others. Increased wave height and closer proximity to the source were associated with higher mortality levels whereas earthquake magnitude was not associated mortality. A number of other factors that were not examined in this study have been shown to influence tsunami damage and impacts including wave velocity, water depth and submarine topography 10. Ecological assessments such as this review may mask significant in-country differences in mortality risk (e.g. population density, rural or urban location, geographic variations and individual-level socio-demographic factors).
Findings from the systematic literature review of studies examining tsunami-related mortality and injury contribute to understanding the primary causes of death and types of injury, as well as factors that place certain populations at increased risk. The most common cause of tsunami-related death was drowning, and the most frequently reported injuries included wounds and lacerations, fractures, and near drowning and/or aspiration. When reported the mortality risk was higher among females and the very young and old and injuries were more common among middle-aged men. Additional mortality risk factors included location during the event and fisheries-based livelihood. Few studies assessed or found relationships between socioeconomic status and mortality risk, although that one study found an inverse association between education level and mortality 28 which suggests that low socioeconomic status may place individuals at increase mortality risk. This suggests that preparedness efforts target specific population groups for the prevention of deaths and injuries. Future studies on both tsunami-related injury and mortality risk would benefit from incorporating additional socio-demographic measures to gain a more comprehensive understanding of risk factors.
A number of strategies could be adopted by the international community and vulnerable countries to mitigate the short and long term impacts of future tsunami events. In the 1998 Papua New Guinea tsunami factors that contributed to higher mortality during this event included concentration of populations in vulnerable areas and failure of residents in affected areas to timely evacuate. In contrast, deployment of medical assistance and international support immediately following the tsunami played a large role in preventing further loss of life 13.With respect to public health in particular, a greater focus on ongoing disease surveillance, the appropriate targeting of aid to those in most need, and strengthening of health care systems 11 can help to mitigate the medium to long term health impacts of tsunamis. Advanced tsunami warning systems may vastly improve early detection, and education campaigns can play a crucial role in improving awareness about tsunami risk and mitigation 10. Policies enacted by the Sri Lankan government following the 2004 tsunami highlight some of the challenges to longer term disaster mitigation where enactment of a buffer zone policy that forced the relocation of coastal communities had deleterious social and economic impacts 12. In adopting disaster mitigation policy, governments should consider the contribution not only of physical vulnerability (i.e. distance of communities from coastal areas) but also social vulnerability, such as livelihoods, to increased disaster risk and the potential short and long term impacts such policies may have on affected communities.
Limitations
Systematic reviews face numerous limitations. The effects of tsunamis are the subject of gross approximations and aggregations which result in a great deal of imprecision. The availability and quality of data has likely increased and improved over time, however, in many events deaths are unknown or unrecorded. For a significant number of events no data are reported for injured, displaced, and affected populations; this likely contributes to a substantial underestimation of the impacts of tsunamis on human populations. Inconsistencies and errors were common in the data files from the two different sources, and in some cases inclusion criteria were not ideal for the purposes of this review which created a challenge in reconciling event lists. Additionally, mainly due to the small number of tsunami run-up events reported over the study period, we were unable to perform more complicated statistical analyses that would have provided estimates of the independent effects of place and event characteristics on tsunami related death. When combined with the relatively small number of tsunami events, uncertainty in the historical record limits the conclusions that can be drawn about the impact of tsunamis on human populations. A principal limitation of the literature review is the fact that only English language publications were included; this likely contributed to incomplete coverage of studies published in other languages originating from low and middle income countries.
Conclusions
From 1900 to 2009, a total of 250,000 tsunami-related deaths and close to 50,000 injuries, respectively, were reported, the majority of which were concentrated in the 2004 Indian Ocean tsunami. An estimated 2.5 million people were affected by tsunamis during this time period. While mortality estimates presented in this study are consistent with those reported in other studies, particularly for the 2004 Indian Ocean Tsunami, the injury figure may be an underestimate of the true value given low reporting levels. The distribution of tsunami related deaths varied greatly by region and economic development level. Findings from the historical event review indicate that the South East Asian region and poorer countries were more likely to experience higher mortality was associated with larger wave height and closer proximity to the source.
The primary cause of tsunami-related mortality was drowning and, although a number of injury types were reported following tsunamis, the ratio of dead to injured is much greater in tsunamis as compared to other natural disaster types. Risk factors for tsunami-related death included female sex and very young and old age. Tsunami losses are likely to increase in future years due to population growth in high risk seismic areas. Increased attention to tsunami prevention and mitigation strategies, with a focus on areas most prone to tsunamis and populations at greater risk is necessary. While strategies that are specific to the development level and country context are important, global initiatives such as early warning systems are essential for further tsunami risk mitigation.
Competing Interests
The authors have declared that no competing interests exist.
Correspondence
Shannon Doocy, Johns Hopkins Bloomberg School of Public Health, 615 N. Wolfe St, Suite E8132, Baltimore, MD 21230. Tel. 410-502-2628. Fax: 410-614-1419. Email: [email protected].
Acknowledgements
We are grateful to Sarah Bernot, Dennis Brophy, Georgina Calderon, Erica Chapin, Joy Crook, Anna Dick, Anjali Dotson, Charlotte Dolenz, Rachel Favero, Annie Fehrenbacher, Janka Flaska, Homaira Hanif, Sarah Henley-Shepard, Marissa Hildebrandt, Esther Johnston, Gifty Kwakye, Lindsay Mathieson, Siri Michel, Karen Milch, Sarah Murray, Catherine Packer, Evan Russell, Elena Semenova, Fatima Sharif, and Michelle Vanstone for their involvement in the systematic literature review and historical event review compilation. We would also like to thank John McGready for biostatistical support, Claire Twose for assistance in designing and implementing the systematic literature review, and Hannah Tappis and Bhakti Hansoti for their assistance in the revision process.Appendix 1
PRISMA Checklist
References
- University of Washington, Dept. of Earth Sciences and Space Sciences. “Tsuanmi!” Last update: March 29, 2005. Available at https://www.ess.washington.edu/tsunami/index.html. Accessed December 15, 2009.
- Keller, E and Blodgett R. (2008). Natural Hazards: Earth’s Processes as Hazards, Disasters, and Catastrophes. Pearson Education: Upper Saddle River, NJ.
- National Oceanic and Atmospheric Administration (NOAA). (2009). Physics of Tsunamis. National Weather Service West Coast and Alaska Tsunami Warning Center Online. Available at: https://wcatwc.arh.noaa.gov/about/physics.htm. Accessed December 15, 2009.
- Noji E. (1997.) Earthquakes. In: Public Health Consequences of Disasters, E. Noji, ed. Oxford University Press, New York, NY.
- McCarty D. (2002). Tsunamis. Hogan D and Burstein J (Eds). Disaster Medicine. Lippincott William and Wilkins: Philadelphia, PA, p229-34.
- EM-DAT the International Disaster Database. (2011). Available at: https://www.emdat.be/disaster-profiles. Accessed June 2, 2011.
- Keim M. (2006). Cyclones, tsunamis and human health: the key role of preparedness. Oceanography 19(2):41-49.
- National Oceanic and Atmospheric Administration (NOAA). NOAA/WDC Historical Tsunami Database at NGDC. Available at: https://www.ngdc.noaa.gov/hazard/tsu_db.shtml
- StataCorp. Chicago, IL. Stata Statistical Software: Release 11.0.
- Levy J and Gopalakrishnan C. (2005). Promoting Disaster-resilient Communities: The Great Sumatra–Andaman Earthquake of 26 December 2004 and the Resulting Indian Ocean Tsunami. Intl J Water Res Dev 21(4):543-559.
- Llewellyn M. (2006). Floods and Tsunamis. Surg Clin N Am 86:557-578.
- Ingram J, Guillerm F, Rio C, et al. (2006). Post-disaster recovery dilemmas: challenges in balancing short-term and long-term needs for vulnerability reduction. Env Sci Pol 9(7-8):607-613.
- Dengler L and Preuss J. (2003). Mitigation Lessons from the July 17, 1998 Papua New Guinea Tsunami. Pure and Applied Geophysics 160(10-11):2001-2031.
- Centers for Disease Control (CDC). (2004). The health effects of tsunamis. Updated December 31, 2004. Available at https://www.bt.cdc.gov/disasters/tsunamis/healtheff.asp. Accessed June 2, 2011.
- Tsuji Y, Imamura F, Matsutomi H, et al. (1995). Field Survey of the East Java Earthquake and Tsunami of June 3, 1994. Pure and Applied Geophysics 144(3-4):839-854.
- Tsuji Y, Matsutomi H, Imamura F, et al. (1995). Damage to Coastal Villages due to the 1992 Flores Island Earthquake Tsunami. Pure and Applied Geophysics 144(3-4):481-524.
- Davies H, Davies J, Perembo C, et al. (2003). The Aitape 1998 Tsunami: Reconstructing the Event from Interviews and Field Mapping. Pure and Applied Geophysics 160(10-11):1895-1922.
- Brennan R. (2005). Rapid health assessment in Aceh Jaya District, Indonesia, following the December 26 tsunami. Emerg Med Australas 17(4):341-350.
- Calder J and Mannion S. Orthopaedics in Sri Lanka post-tsunami. (2005). Journal of Bone and Joint Surgery 87(6):759-76.
- Johnson L and Travis A. (2006). Trauma response to the Asian tsunami: Krabi Hospital, Southern Thailand. Emerg Med Australas 18(2):196-8.
- Lee V, Low E, Ng et al. (2005). Disaster relief and initial response to the earthquake and tsunami in Meulaboh, Indonesia. Ann Acad Med Singapore 34(9):586-90.
- Lim J, Yoon D, Jung G, et al. (2005). Medical needs of tsunami disaster refugee camps. Fam Med 37(6):422-8.
- Maegele M, Gregor S, Steinhausen E, et al. (2005). The long-distance tertiary air transfer and care of tsunami victims: injury pattern and microbiological and psychological aspects. Crit Care Med 33(5):1136-40.
- Chambers A, Campion M, Courtenay B, et al. (2006). Operation Sumatra Assist: surgery for survivors of the tsunami disaster in Indonesia. ANZ J Surg 76(1-2):39-42.
- Fan S. (2006). Clinical cases seen in tsunami hit Banda Aceh: from a primary health care perspective. Ann Acad Med Singapore. 35(1):54-9.
- Kwak Y, Shin S, Kim K. (2006). Experience of a Korean disaster medical assistance team in Sri Lanka after the South Asia tsunami. J Korean Med Sci 21(1):143-50.
- Centers for Disease Control and prevention (CDC). Assessment of health-related needs after tsunami and earthquake--three districts, Aceh Province, Indonesia, July-August 2005. MMWR Morb Mortal Wkly Rep 55(4):93-7.
- Nishikiori N, Abe T, Costa D, et al. (2006). Who died as a result of the tsunami? Risk factors of mortality among internally displaced persons in Sri Lanka: a retrospective cohort analysis. BMC Public Health. 20;6:73.
- Nishikiori N, Abe T, Costa D, et al. (2006). Timing of mortality among internally displaced persons due to the tsunami in Sri Lanka: cross sectional household survey. BMJ. 332(7537):334-5.
- Redwood-Campbell L and Riddez L. (2006). Post-tsunami medical care: health problems encountered in the International Committee of the Red Cross Hospital in Banda Aceh, Indonesia. Prehosp Disaster Med 21(1):s1-7.
- Rodriguez H, Watchendorf T, Kendra J et al. (2006). A snapshot of the 2004 Indian Ocean tsunami: societal impacts and consequences. Disaster Prevention and Management 15(1):163-177.
- Rofi A, Doocy S, and Robinson C. (2006). Tsunami mortality and displacement in Aceh province. Disasters 30(3): 340-350.
- Roy N. (2006). The Asian Tsunami: PAHO disaster guidelines in action in India. Prehosp Disaster Med 21(5):310-5.
- van Griensven F, Chakkraband ML, Thienkrua W et al. (2006). Mental health problems among adults in tsunami-affected areas in southern Thailand. JAMA 296(5):537-48.
- Yamada S, Gunatilake R, Roytman T, et al. (2006). The Sri Lanka tsunami experience. Disaster Manag Response 4(2):38-48.
- Doocy S, Gorokovich Y, Burnham G, Balk D, and Robinson C. (2007). Tsunami mortality estimation and vulnerability mapping in Aceh, Indonesia. American Journal of Public Health 97(S1): 146-51.
- Doocy S, Rofi A, Moodie C, Spring E, Bradley S, Burnham G, and Robinson C. (2007). Tsunami mortality in Aceh Province, Indonesia. Bulletin of the World Health Organization 85(2): 273-278.
- Johnson L and Travis A. (2006). Trauma response to the Asian tsunami: Krabi Hospital, Southern Thailand. Emerg Med Australas 18(2):196-8.
- Johnson L and Travis A. (2006). Trimodal death and the injuries of survivors in Krabi Province, Thailand, post-tsunami. ANZ J Surg 76(5):288-9.
- Meynard J, Nau A, Halbert E et al. (2008). Health indicators in children from Meulaboh, Indonesia, following the tsunami of December 26, 2004. Mil Med. 173(9):900-5.
- Prasartritha T, Tungsiripat R, and Warachit P. (2008). The revisit of 2004 tsunami in Thailand: characteristics of wounds. Int Wound J. 5(1):8-19.
- Doocy S, Robinson C, Moodie C and Burnham G. (2009). Tsunami-related injury in Aceh Province, Indonesia. Global Public Health 4(2):205-214.
- Doung-ngern P, Vatanaprasan T, Chungpaibulpatana J et al. (2009). Infections and treatment of wounds in survivors of the 2004 Tsunami in Thailand. Int Wound J 6(5):347-54.
- Nagamatsu S, Maekawa T, Ujike Y, Hashimoto S, Fuke N. The earthquake and Tsunami- observations by Japanese physicians since the 11 March catastrophe. Critical Care. 2011, 15:167.
Leave a Comment
You must be logged in to post a comment.