Abstract
Background: Our objective was to identify published models of coordination between entities funding or delivering health services in humanitarian crises, whether the coordination took place during or after the crises.
Methods: We included reports describing models of coordination in sufficient detail to allow reproducibility. We also included reports describing implementation of identified models, as case studies. We searched Medline, PubMed, EMBASE, Cochrane Central Register of Controlled Trials, CINAHL, PsycINFO, and the WHO Global Health Library. We also searched websites of relevant organizations. We followed standard systematic review methodology.
Results: Our search captured 14,309 citations. The screening process identified 34 eligible papers describing five models of coordination of delivering health services: the “Cluster Approach” (with 16 case studies), the 4Ws “Who is Where, When, doing What” mapping tool (with four case studies), the “Sphere Project” (with two case studies), the “5×5” model (with one case study), and the “model of information coordination” (with one case study). The 4Ws and the 5×5 focus on coordination of services for mental health, the remaining models do not focus on a specific health topic. The Cluster approach appears to be the most widely used. One case study was a mixed implementation of the Cluster approach and the Sphere model. We identified no model of coordination for funding of health service.
Conclusion: This systematic review identified five proposed coordination models that have been implemented by entities funding or delivering health service in humanitarian crises. There is a need to compare the effect of these different models on outcomes such as availability of and access to health services.
Funding Statement
We would like to thank the Alliance for Health Policy and Systems Research for supporting the work of our group on systematic reviews related to health policy and health systems. We would also like to thank the National Council for Scientific Research (CNRS) for supporting this work. Conflict of interest: The authors have declared that no competing interests exist.Notice of Corrections
[10 Feb 2017]: PLOS Currents – Correction: Lotfi T, Bou-Karroum L, Darzi A, Hajjar R, El Rahyel A, El Eid J, et al. Coordinating the Provision of Health Services in Humanitarian Crises: a Systematic Review of Suggested Models. PLOS Currents Disasters. 2016 Aug 3. Edition 1. doi: 10.1371/currents.dis.95e78d5a93bbf99fca68be64826575fa. View Correction.
Background
National and international humanitarian relief organizations play a significant role in humanitarian crises.1,2 For example, after the Asian Tsunami in 2004, relief operations involved the government institutions of the concerned countries, Non-Government Organizations (NGOs), United Nations (UN) agencies, and disaster relief teams from aiding nations3 with an estimated total number of over a 1000 actors.4 Coordination between these organizations in planning and adapting policies is essential to cope with these crises and enhance the ability to deal with them.5
There is evidence of lack of coordination between organizations providing health services in public health emergencies.4,6 For example, the lack of coordination between stakeholders complicated food delivery in the humanitarian crises in Iraq, Darfur and Palestine.7 Another example is the response to the Haiti earthquake, which was described as worst natural disaster in modern history, that lacked coordination and resources.8
Studies have reported the importance of providing adequate support to the relevant national authorities at the beginning of a humanitarian crisis in order to optimize the use of available resources to establish a coordination mechanism.7 Allowing stakeholders to work collectively creates an enabling environment for coordinating both information and action, facilitating the implementation of effective interventions and the provision of equitable assistance to those in need.7,9,10
Major organizations, such as the UN, Red Cross and governmental and non-governmental agencies have attempted to form mechanisms and frameworks of coordination.9 It would be important for a group of organizations contemplating a coordination mechanism, to be aware of and understand the different coordination models.
Our objective was to identify published models of coordination between entities funding or delivering health services in humanitarian crises, whether the coordination took place during or after the crises.
Methods
Eligibility criteria
We included a study irrespective of its design, as long as it provided a detailed description of a coordination process or model. The types of organizations of interest included UN agencies, local and international organizations and agencies including NGOs, governmental agencies and bodies. We included different settings such as humanitarian crises, whether the coordination took place during or after the crises. We did not exclude studies that were not published in English.
Search strategy
We registered a protocol for this review in PROSPERO International prospective register of systematic reviews under number PROSPERO2014:CRD42014009267. We used the electronic databases (Medline, PubMed, EMBASE, Cochrane Central Register of Controlled Trials, CINAHL, PsycINFO, and the WHO Global Health Library) and websites of relevant organizations to run our search strategy (Appendix 1). We did not use any language restrictions.
Selection of studies
We followed the standard systematic review methodology: we screened the titles and abstracts of identified citations for potential eligibility in duplicate and independently. We retrieved the full texts of citations considered as potentially eligible by at least one of the two reviewers. Then, we screened the full texts in duplicate and independently for eligibility. We resolved disagreements by discussion or with the help of a third reviewer. We used a standardized and pilot tested screening form and completed calibration exercises.
Data collection
We abstracted data independently and in duplicate using standardized and pilot tested data abstraction form. We resolved disagreements by discussion or with the help of a third reviewer. We abstracted the following data: the study ID, the name of the model, the setting it was implemented in, and the description of the model.
Data synthesis
Given the qualitative nature of the data, we synthesized and reported the findings narratively. First, we narratively described both the full and partial coordination models. Full coordination models refer to models that attempted to cover all aspects of interaction between corresponding agencies and bodies while partial models covered only one aspect of interaction such as information coordination. In addition we presented in a tabular format the case studies relevant to each of these models.
Results
Selection of studies
Figure 1 shows the study flow. Of the 14,309 citations identified by the electronic literature search, 34 papers met our inclusion criteria and described five models of coordination of delivering health services: the Cluster approach8,9,11–32 ; the 4Ws “Who is Where, When, doing What” mapping tool 33–36; the Sphere project 9,23,37,38; the 5×5 model 39; and a model of information coordination40. We did not identify any model of coordination for funding health services. We excluded 412 papers for the following reasons: not dealing with a model of coordination (n=311); not describing how coordination was done (n= 4); conference abstracts (n= 99).

Fig. 1: Study Flow Diagram
We describe below the five models in full details. Table 1 compares the main characteristics of the five models. Appendix 2 presents the identified case studies for the different models: the Cluster approach (n=16); 4Ws (n=4); the Sphere project (n=2); the 5×5 model (n=1) and the model of information coordination (n=1).
Table 1. Comparison of the main characteristics of five coordination models. (IASC: Inter-Agency Standing Committee; NGOs: Non-Governmental Organizations; ICRC: International Red Cross and Red Crescent; PIH: Partners in Health; CDC: Center for Disease Control and Prevention)
The cluster approach
In 1992, key UN and non-UN humanitarian partners, established the Inter-Agency Standing Committee (IASC) as the “primary mechanism for inter-agency coordination of humanitarian assistance”. In 2005, the IASC worked with the UN Emergency Relief Coordinator to develop the cluster approach as a “way of organizing coordination and cooperation among humanitarian actors to facilitate joint strategic planning”.11–13,31,32 The Cluster aims to support and match the efforts of national authorities in critical areas of preparedness and response within a framework of agreed objectives. It also aims to avoid gaps and/or overlap in the resources and international humanitarian response.
Figure 2 shows how the Cluster system works. A Cluster forms at the country level under the overall leadership of the humanitarian coordinator, and includes multiple national and international agencies working together within a specific sector of emergency response. A Cluster Lead Agency (CLA) is assigned for each sector: United Nations Children’s Fund (UNICEF) for nutrition and for water and sanitation, the World Health Organization (WHO) for health, and the United Nations High Commissioner for Refugees (UNHCR) and the International Federation for Red Cross and Red Crescent (IFRC) for emergency shelter. Moreover, the lead agency or co-lead agencies are held accountable, through this approach, for the performance of their cluster by being responsible to ensure adequate coordination of activities by partners involved in its specified area.29 Figure 3 shows the inter-organizational functioning of a Cluster approach with further narrative details provided in Appendix 3.
Photo credit: Office for the Coordination of Humanitarian Affairs49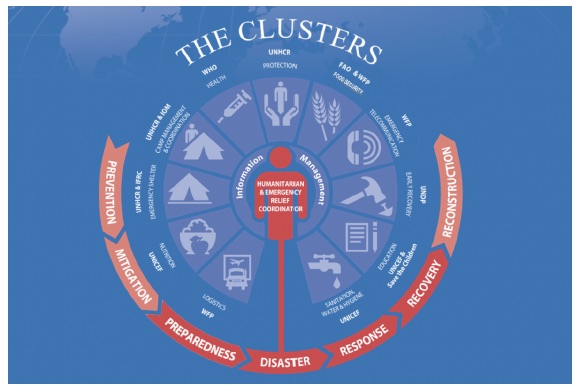
Fig. 2: Diagram illustrating how the Cluster system works
(IDPs = Internally Displaced Persons; OCHA = UN Office for Coordinating Humanitarian Affairs)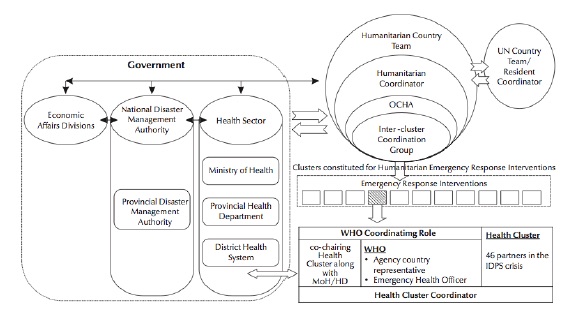
Fig. 3: Inter-organizational functioning of a Cluster approach Humanitarian health response coordination framework in Pakistan
Appendix 2 describes 16 papers reporting on 19 case studies where the Cluster approach was implemented.
The 4Ws
In 2007, the IASC developed through its Reference Group on Mental Health and Psychosocial Support (MHPSS) the “Who is Where, When, doing What” (4Ws) tool.33 The IASC developed this tool to help in the coordination of responsibilities between the MHPSS actors responding to the Iraqi refugees crisis in Jordan following the 2003 Iraqi war.
The 4Ws tool included a one-page introduction and three activity spreadsheets: one for information about the organization, one for details of activities, and the last one for 11 pre-defined MHPSS activities and corresponding sub-activities.34,36,41 Three mapping exercises were conducted, and aimed to: 1) Map MHPSS activities in Jordan; 2) Recommend changes to the tool, based on field experience; 3) Present the findings of the mapping to the Jordan MHPSS Coordination Group.36 After each mapping exercise, adjustments were made to the activity spreadsheet.36
As an illustrative example, and in the case of Jordan, the tool identified the following:36
The IASC provides a guide on when and how to apply this tool (Appendix 4).33
The Sphere Project
In 1997, a group of NGOs and the International Red Cross and Red Crescent (ICRC) Movement developed the Sphere Project following the 1994 Rwandan genocide. The project aim was to provide guidance for humanitarian responders in all sectors.27 It is considered the “first collaborative initiative to produce globally applicable minimum standards for humanitarian response”. Sphere encourages providing a coordination framework between governmental organizations for international and local disaster relief. 22,38,42
The Sphere project developed a tool for “field-based inter-agency coordination” which consisted of: 1) binding principles of engagement; 2) protocol for assumption of responsibilities; 3) health-sector gap identification and 4) health-sector components summaries. The project also identified a set of “minimum standards in health action” for evidence-based and sector-wide consensus on best practices in humanitarian response. Appendix 5 lists the key actions in leadership and coordination, part of those minimum standards.
5×5 model
In the aftermath of the Haiti earthquake, Haitian and American nationals working for Partners in Health (PIH) developed the “5×5” intervention model to manage mental health services delivered by their organization.39 The name of the intervention refers to five key “skill packages” and five “implementation rules”.
The five key “skill packages” aim to provide mental health-specific platform to apply algorithms for common disorders. These packages are consistent with the WHO mental health intervention guide in non-specialist health settings and include: 1) case finding, engagement, follow-up, and psycho-education; 2) targeted psychological interventions; 3) medication management; 4) supervision and consultation; 5) quality oversight.
The five “implementation rules” consist of the following: 1) assess context first; 2) identify priority care pathways; 3) specify decision-support tools, supervision, and triage rules; 4) use quality-improvement practices; 5) plan for sustainability and capacity building; and thus the name 5×5 model.
A model of information coordination
In 2004, and in response to the Tsunami of the shores of the Indian Ocean, the Center for Disease Control and Prevention (CDC) formed the Responder Resilience and Mental Health Team to contribute to the humanitarian relief efforts.40 Because of the complex relief efforts, there was a need for coordination between partners through the Internet and occasional ship-to-shore teleconferences. It was important to inform the emergency operations command about the psychosocial relief efforts through reports, critical resource documents on traumatic exposure metrics and intervention manuals with intervention mapping strategies.
Coordination for funding health services
Although we did not identify any model of coordination for funding health services, we identified one paper discussing coordinating funds in humanitarian crises. This paper presented the results of a conference held by WHO in Phuket, Thailand, May 2005 to assess the Health Aspects of the Tsunami Disaster in Asia, December 2004. One problem relied in managing the outpouring resources of aid. Four recommendations were brought up in this conference: 1) to create a financial monitoring system reliable and cost-effective for all stakeholders; 2) to require targeted funding and address constraints of pooled funding; 3) to compare the Tsunami funding to principles of best practices and evaluate it; 4) to better coordination within and across organizations and between donors.43
Discussion
Our systematic review aimed to identify models of coordination between entities funding or delivering health services in humanitarian crises.
We found five models of coordination of delivering health services and no model of coordination for funding these services. While the 4Ws and the 5×5 focus on coordination of services for mental health, the remaining models do not focus on a specific health topic. The Cluster approach appears to be the most widely used, at least based on the number of identified case studies using it (n=16 out of 24). The Sphere Project was used along with the cluster approach in one case study.
There might be different explanations for why the Cluster approach was the most widely reported to be used. First, it is the first approach to have been developed and reported. Second, the developer of the approach being the UN system has probably given it more visibility than other approaches. In addition, there is some evidence that this approach may improve coordination among organizations, particularly those working on sexual and reproductive health.47
In fact, our group has produced one systematic review assessing the effectiveness of models of coordination.44 The review identified only four evaluation studies providing very low quality evidence,45–48 and only one of these assessed a formally defined coordination model, which was the cluster approach.47 Those studies found that information coordination may be effective in improving health systems inputs; and that management coordination (e.g., with the cluster model) may improve health system inputs and access.44
Our study has a number of strengths. First, it is the first study describing models for coordinating health services in humanitarian crises. Second, we followed a systematic review methodology, including a search of non-peer reviewed literature. One limitation of the study is the exclusion of non-English published papers. However, it is unlikely that an eligible study was published in a language different than English given the usual involvement of international organization in these situations.
While the authors of the models call for using them across emergency settings, the case studies suggest a potential pattern for using certain models for specific types of emergencies. For example, the Cluster and 4Ws approaches have been used in emergencies related to both war and natural disasters while the rest of the models have been reportedly used only in emergencies related to natural disasters.
Irrespective of the specific coordination model, their use in general might be challenging during or in the aftermath of humanitarian crises for a number of reasons. The nature of the crisis itself and the urgency to deliver services might not allow organizations to dedicate the needed time or resources to coordinate their efforts. Also, these organizations might not be aware of such models, or might not have the needed expertise to implement them. Finally, the cultures of the individual organizations might conflict and negatively affect any will or effort to coordinate.
In conclusion, five coordination models have been implemented worldwide in different disasters in order to coordinate the delivery of health services. These results should serve policymakers, and administrators of entities delivering health services during and post-humanitarian crises to choose from a number of options on how to coordinate their efforts. It is challenging to provide specific guidance on which model to use. However, we suggest that decision makers prioritize models that, based on the presented case studies, have been used in settings similar to theirs, such as the type of disaster or the countries in which the crisis is taking place.
There is a need to conduct further research to assess the effectiveness and efficiency of the identified models, specifically in terms of availability of healthcare services and access to health services.
Appendices
Appendix 1: Medline, EMBASE, Scopus, CINAHL, WHO Global Health Library, PsychInfo, and Cochrane Search strategies
Medline
Database: Ovid MEDLINE(R) <1946 to March Week 1 2014>
Search Strategy:
1 exp Refugees/ (6558)
2 refugee*.ti,ab. (5394)
3 exp War/ (30340)
4 (war or wars).ti,ab. (25791)
5 disasters/ or exp disaster planning/ or exp emergency shelter/ or exp mass casualty incidents/ (23240)
6 (disaster* or tsunami* or earthquake* or volcan* or hurricane* or cyclone*).ti,ab. (20082)
7 (mass adj2 casualt*).ti,ab. (1355)
8 exp earthquakes/ or exp tsunamis/ or exp volcanic eruptions/ (2728)
9 ((conflict* adj3 (area* or zone* or setting* or region)) or (conflict-affected adj3 (area* or zone*or setting* or region)) or armed-conflict* or (armed adj3 conflict*) or (conflict adj3 ethnic) or post-conflict or postconflict or (military adj3 conflict) or “post conflict”).ti,ab. (1770)
10 ((internal* adj2 (displace* or dis-place*)) or (forcibl* adj2 (displace* or dis-place*))).ti,ab. (422)
11 or/1-10 (84689)
12 (coordinat* or co-ordinat* or cooperat* or co-operat* or collaborat*).ti,ab. (297694)
13 exp cooperative behavior/ (28026)
14 international cooperation/ or medical missions, official/ (39498)
15 or/12-14 (346524)
16 organizations/ or exp charities/ or government/ or exp “united states dept. of health and human services”/ or exp local government/ or exp state government/ or exp government agencies/ or exp international agencies/ or organizations, nonprofit/ or foundations/ or voluntary health agencies/ (155048)
17 ((international or government* or non-government* or nongovernment* or nonprofit or non-profit or donor*) adj2 (organization* or organisation* or agenc* or bodies or foundation*)).ti,ab. (15316)
18 (united adj nation*).ti,ab. (3232)
19 (red adj cross).ti,ab. (2727)
20 (“world health” adj (organization or organisation)).ti,ab. (26650)
21 exp relief work/ or exp rescue work/ (4857)
22 ((relief or rescue) adj (work or effort*)).ti,ab. (395)
23 ((foreign or humanitarian) adj2 (aid or aids)).ti,ab. (497)
24 or/16-23 (193928)
25 15 and 24 (18828)
26 ((health adj3 (cluster* or inter-cluster or zone*)) or (cluster adj2 approach)).ti,ab. (952)
27 25 or 26 (19765)
28 11 and 27 (2006)
EMBASE
Database: EMBASE <1980 to 2014 Week 10>
Search Strategy:
1 exp refugee/ (7321)
2 refugee*.ti,ab. (6074)
3 disaster/ or mass disaster/ or natural disaster/ or disaster planning/ (26347)
4 (disaster* or tsunami* or earthquake* or volcan* or hurricane* or cyclone*).ti,ab. (27440)
5 (mass adj2 casualt*).ti,ab. (1621)
6 exp earthquake/ (5038)
7 exp tsunami/ (1424)
8 exp volcano/ (2135)
9 war/ (24617)
10 (war or wars).ti,ab. (29491)
11 ((internal* adj2 (displace* or dis-place*)) or (forcibl* adj2 (displace* or dis-place*))).ti,ab. (548)
12 ((conflict* adj3 (area* or zone* or setting* or region)) or (conflict-affected adj3 (area* or zone*or setting* or region)) or armed-conflict* or (armed adj3 conflict*) or (conflict adj3 ethnic) or post-conflict or postconflict or (military adj3 conflict) or “post conflict”).ti,ab. (2216)
13 or/1-12 (92212)
14 (coordinat* or co-ordinat* or cooperat* or co-operat* or collaborat*).ti,ab. (376241)
15 exp cooperation/ (39554)
16 coordination/ (3306)
17 exp international cooperation/ (157714)
18 or/14-17 (550057)
19 exp non profit organization/ (21069)
20 ((international or government* or non-government* or nongovernment* or nonprofit or non-profit or donor*) adj2 (organization* or organisation* or agenc* or bodies or foundation*)).ti,ab. (20577)
21 (united adj nation*).ti,ab. (4259)
22 (red adj cross).ti,ab. (3471)
23 (“world health” adj (organization or organisation)).ti,ab. (33513)
24 red cross/ (2731)
25 United Nations/ (6687)
26 world health organization/ (66809)
27 rescue work/ (573)
28 relief work/ (859)
29 ((relief or rescue) adj (work or effort*)).ti,ab. (466)
30 ((foreign or humanitarian) adj2 (aid or aids)).ti,ab. (454)
31 or/19-30 (136509)
32 18 and 31 (28322)
33 ((health adj3 (cluster* or inter-cluster or zone*)) or (cluster adj2 approach)).ti,ab. (1271)
34 32 or 33 (29576)
35 13 and 34 (2523)
Scopus
Search Strategy:
((TITLE-ABS-KEY(refugee* OR disaster* OR earthquake* OR tsunami* OR hurricane* OR cyclone*or war OR wars OR conflict OR conflicts OR post-conflict)) OR (TITLE-ABS-KEY(internal* W/2 displace*)) OR (TITLE-ABS-KEY(forcibl* W/2 displace*)) OR (TITLE-ABS-KEY(mass W/2 casualt*))) AND (((TITLE-ABS-KEY(coordinat* OR co-ordinat* OR cooperat* OR co-operate* OR collaborat*)) AND (((TITLE-ABS-KEY((international OR government* OR non-government* OR nongovernment* OR nonprofit OR non-profit OR donor*) W/2 (organization* OR organisation* OR agenc* OR bodies OR foundation*))) OR (TITLE-ABS-KEY(united W/0 nation*)) OR (TITLE-ABS-KEY(red W/0 cross)) OR (TITLE-ABS-KEY(“world health organization” OR “world health organisation”))) OR (TITLE-ABS-KEY(foreign W/1 aid)) OR (TITLE-ABS-KEY(humanitarian W/1 aid)) OR (TITLE-ABS-KEY(rescue W/1 (work OR effort*))) OR (TITLE-ABS-KEY(relief W/1 (work OR effort*))))) OR (TITLE-ABS-KEY(health W/2 cluster)))
CINAHL
Search strategy:
S12 S1 AND S11
S11 S7 OR S8 OR S9
S10 ((health N2 (cluster* or inter-cluster or zone*)) or (cluster N1 approach)) AND (S8 OR S9)
S9 (health N2 (cluster* or inter-cluster or zone*)) or (cluster N1 approach)
S8 international N2 cooperation
S7 S2 AND S6
S6 (S3 OR S4 OR S5)
S5 (rescue N2 work) or (relief N2 (work or effort*)) or (foreign N2 (aid or aids)) or (humanitarian N2 (aid or aids))
S4 “united nation*” or “red cross” or (world health N1 (organization or organization))
S3 (international or government* or non-government* or nongovernment* or nonprofit or non-profit or donor*) N2 (organization* or organisation* or agenc* or bodies or foundation*)
S2 coordinat* or co-ordinat* or cooperat* or co-operat* or collaborat*
S1 refugee* or (internal* N2 displace*) or (forcibl* N2 displace*) or war or wars or conflict or conflicts or disaster* or (mass N2 casualt*) or tsunami* or earthquake* or volcan* or hurricane* or cyclone*
WHO Global Health Library, PsycInfo and Cochrane
Search strategy:
(refugee* or disaster* or war or wars or conflict or conflicts or post-conflict or internal* displace* or forcibl* displace* or mass casualt* or earthquake* or tsunami* or volcan*) AND ((coordinat* or co-ordinat* or cooperat* or co-operat* or collaborat*) and (foreign aid or humanitarian aid or rescue work or relief work or relief effort or ((international or government* or non-government* or nongovernment* or nonprofit or non-profit or donor*) AND (organization* or organisation* or agenc* or bodies or foundation*))))
Appendix 2: Case studies by model
The Cluster Approach (* Used both the Cluster approach and the Sphere approach)
The Cluster Approach (Continued) (* Used both the Cluster approach and the Sphere approach)
The 4Ws
The Sphere Project
The 5×5 Model
The Information coordination Model
Appendix 3: Functioning of a Cluster Lead Agency
A country-level Health Cluster includes the organizations providing health services in affected areas and the main health-sector stakeholders. In order to build on local capacities and help develop and sustain relations with relevant government and organizations involved in health-related activities, a Health Cluster lead agency bridges between the national and international actors. Ministry of health leads the coordination process in settings where it is in a strong position. In settings where the capacity of the Ministry of health to lead is compromised (such as in ongoing conflict areas), practical arrangements are made, and most of the times a ministry representative and the Cluster Lead Agency (CLA) co-chair meetings. The United Nations Office for the Coordination of Humanitarian Affairs (OCHA) is in charge of coordinating the response of the UN system to major emergencies . OCHA works closely with global lead agencies and NGOs in developing their policies and coordinating inter-cluster issues and ensures efficient system functioning on the field.
Appendix 4: Tool used for the application of “Who is Where, When, doing What”
Tool used for the application of “Who is Where, When, doing What”
Appendix 5: The Sphere’s key actions in leadership and coordination, part of the ‘minimum standards in health action’
– Ensure that representatives of the Ministry of Health (MOH) lead or at the very least are closely involved in the health sector coordination, whenever possible;
– When the MOH lacks the necessary capacity or willingness to provide leadership in the response, an alternate agency with the requisite capacity must be identified to take the lead in health sector coordination;
– Hold regular health coordination meetings for local and external partners at central, sub-national and field levels within the health sector, and between health and other sectors and appropriate cross-cutting theme groups;
– Clarify and document the specific responsibilities and capacities of each health agency to ensure optimal coverage of the population;
-Establish working groups within the health coordination mechanism whenever a particular situation may require it (e.g. outbreak preparedness and response, reproductive health);
– Regularly produce and disseminate updates and health sector bulletins.
Acknowledgements
We would like to thank Ms. Aida Farha for assisting in developing the search strategy.References
- Beigbeder, Y., The Role and Statuts of International Humanitarian Volunteers and Organizations: The Right and Duty to Humanitarian Assistance. Vol. 12. 1991: Martinus Nijhoff Publishers.
- Balcik, B., et al., Coordination in humanitarian relief chains: Practices, challenges and opportunities. International Journal of Production Economics, 2010. 126(1): p. 22-34.
- Chia, E.S., Engineering disaster relief. Technology and Society Magazine, IEEE, 2007. 26(3): p. 24-29.
- Lassa, J., Post Disaster Governance, Complexity and Network Theory: Evidence from Aceh, Indonesia After the Indian Ocean Tsunami 2004. PLOS currents Disasters, 2015(1): p. 23.
- Michaud 3rd, E.C. and G.L. Maxwell, Medical capacity building efforts in northern Iraq 2009-2010. Military medicine, 2012. 177(6): p. 676-680.
- Chen, L., et al., Human resources for health: overcoming the crisis. The Lancet. 364(9449): p. 1984-1990.
- Bagchi, K., et al., Nutrition in humanitarian crises. Eastern Mediterranean Health Journal, 2004. 10(6): p. 747-753.
- Kirsch, T., L. Sauer, and D. Guha Sapir, Analysis of the international and US response to the Haiti earthquake: recommendations for change. Disaster Medicine & Public Health Preparedness, 2012. 6(3): p. 200-8.
- Bradt, D.A. and C.M. Drummond, From complex emergencies to terrorism--new tools for health-sector coordination in conflict-associated disasters. Prehospital and disaster medicine : the official journal of the National Association of EMS Physicians and the World Association for Emergency and Disaster Medicine in association with the Acute Care Foundation, 2003. 18(3): p. 263-271.
- Ferguson, E.W., et al., A global health disaster network is needed. BMJ. 310(6991): p. 1412-1412.
- Zoraster, R., Disaster coordination needs more than the "health cluster". Prehospital and disaster medicine : the official journal of the National Association of EMS Physicians and the World Association for Emergency and Disaster Medicine in association with the Acute Care Foundation, 2010. 25(4): p. 372-373.
- Oh, N., A. Okada, and L.K. Comfort, Building Collaborative Emergency Management Systems in Northeast Asia: A Comparative Analysis of the Roles of International Agencies. Journal of Comparative Policy Analysis: Research and Practice, 2014.
- Moszynski, P., Cluster approach improves provision of disaster aid, says WHO. BMJ, 2008. 337: p. a1571.
- Leaning, J. and D. Guha-Sapir, Natural disasters, armed conflict, and public health. N Engl J Med, 2013. 369(19): p. 1836-42.
- Krin, C.S., et al., Disaster management: Appropriate response to humanitarian crises. BMJ (Online), 2010. 340(7741): p. 290.
- Krin, C.S., et al., Appropriate response to humanitarian crises. BMJ, 2010. 340: p. c562.
- Gorry, C., Haiti one year later: Cuban medical team draws on experience and partnerships. MEDICC review, 2011. 13(1): p. 52-5.
- Estupinan-Day, S., C. Lafontant, and M.C. Acuna, Integrating Oral Health into Haiti's national Health plan: From disaster relief To sustainable development. Revista Panamericana de Salud Publica/Pan American Journal of Public Health, 2011. 30(5): p. 484-489.
- Clarke, J.N., Transitional coordination in Sudan (2006-08): lessons from the United Nations Resident Coordinator's Office.[Erratum appears in Disasters. 2013 Jul;37(3):ii]. Disasters, 2013. 37(3): p. 420-41.
- Centers for Disease, C. and Prevention, Rapid establishment of an internally displaced persons disease surveillance system after an earthquake --- Haiti, 2010. MMWR - Morbidity & Mortality Weekly Report, 2010. 59(30): p. 939-45.
- Burkle Jr, F.M., A.D. Redmond, and D.F. McArdle, An authority for crisis coordination and accountability. The Lancet, 2012. 379(9833): p. 2223-2225.
- Bradt, D.A. and C.M. Drummond, Professionalization of disaster medicine--an appraisal of criterion-referenced qualifications. Prehospital and disaster medicine : the official journal of the National Association of EMS Physicians and the World Association for Emergency and Disaster Medicine in association with the Acute Care Foundation, 2007. 22(5): p. 360-368.
- Rosborough, S., A tale of two responses: Haiti earthquake highlights the need for training in international disaster response. Disaster Med Public Health Prep. 4(1): p. 21-3.
- Morris, S., Haiti earthquake: perspectives from the ground and lessons from afar. Disaster medicine and public health preparedness, 2010. 4(2): p. 113-115.
- Bile, K., et al., Learning through crisis: development and implementation of a health cluster strategy for internally displaced persons. 2010.
- Ager, A., et al., Child protection assessment in humanitarian emergencies: Case studies from Georgia, Gaza, Haiti and Yemen. Child abuse & neglect, 2011. 35(12): p. 1045-1052.
- Austin, J., et al., Reproductive health: a right for refugees and internally displaced persons. Reproductive Health Matters, 2008. 16(31): p. 10-21.
- WHO, Country Cooperation Strategy for WHO and Lebanon 2010–2015. WHO EMRO, 2010. ARD/035/E.
- Cumming-Bruce, N., WHO takes lead on health as UN tackles crises. Bulletin of the World Health Organization, 2009. 87(4): p. 250-251.
- Adams, P., Relief agencies prepare for long haul in Haiti. The Lancet, 2010. 375(9714): p. 539.
- Shearer, D. and F. Pickup, Still falling short: protection and partnerships in the Lebanon emergency response. Disasters, 2007. 31(4): p. 336-52.
- Kondaveti, R. and A. Ganz, Decision support system for resource allocation in disaster management. Conference proceedings : .. 2009. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Conference. 2009: p. 3425-3428.
- (IASC), I.-A.S.C.I.R.G.o.M.H.a.P.S.i.E.S., Who is Where, When, doing What (4Ws) in Mental Health and Psychosocial Support. 2012.
- Eloul, L., et al., Inter-agency coordination of mental health and psychosocial support for refugees and people displaced in Syria. Intervention, 2013. 11(3): p. 340-348.
- O’Connell, R., et al., Who is Where, When, doing What: mapping services for mental health and psychosocial support in emergencies. Intervention, 2012. 10(2): p. 171-176.
- Baca, M.J., et al., The development of a comprehensive mapping service for mental health and psychosocial support in Jordan. Intervention, 2012. 10(2): p. 177-187.
- Zoraster, R.M., Barriers to disaster coordination: health sector coordination in Banda Aceh following the South Asia Tsunami. Prehospital and disaster medicine : the official journal of the National Association of EMS Physicians and the World Association for Emergency and Disaster Medicine in association with the Acute Care Foundation, 2006. 21(1): p. s13-18.
- Gostelow, L., The Sphere Project: The implications of making humanitarian principles and codes work. Disasters, 1999. 23(4): p. 316-325.
- Raviola, G., et al., Mental health response in Haiti in the aftermath of the 2010 earthquake: A case study for building long-term solutions. Harvard Review of Psychiatry, 2012. 20(1): p. 68-77.
- Reissman, D.B., et al., The virtual network supporting the front lines: addressing emerging behavioral health problems following the tsunami of 2004. Military medicine, 2006. 171(10): p. 40.
- Babcock, C., et al., Chicago medical response to the 2010 earthquake in Haiti: translating academic collaboration into direct humanitarian response. Disaster medicine and public health preparedness, 2010. 4(2): p. 169-173.
- Bhan, A., Guidelines, planning and training will help in a coordinated disaster response. Natl Med J India, 2006. 19(5): p. 294.
- Procacci, P., et al., Panel 2.4: funding policies and practices. Prehospital and disaster medicine : the official journal of the National Association of EMS Physicians and the World Association for Emergency and Disaster Medicine in association with the Acute Care Foundation, 2005. 20(6): p. 408-411.
- Akl, E.A., et al., Effectiveness of Mechanisms and Models of Coordination between Organizations, Agencies and Bodies Providing or Financing Health Services in Humanitarian Crises: A Systematic Review. PloS one, 2015. 10(9): p. e0137159.
- Celik, S. and S. Corbacioglu, Role of information in collective action in dynamic disaster environments. Disasters, 2010. 34(1): p. 137-154.
- Moore, S., E. Eng, and M. Daniel, International NGOs and the role of network centrality in humanitarian aid operations: a case study of coordination during the 2000 Mozambique floods. Disasters, 2003. 27(4): p. 305-318.
- Landegger, J., et al., Strengths and weaknesses of the humanitarian Cluster Approach in relation to sexual and reproductive health services in northern Uganda. International health, 2011. 3(2): p. 108-114.
- Rahman, M.O. and M. Bennish, Health related response to natural disasters: The case of the Bangladesh cyclone of 1991. Social Science & Medicine, 1993. 36(7): p. 903-914.
- OCHA. How the cluster system works. Coordination Tools [cited 2015 13 November 2015]
Reference Link - Gorry, C., Haiti one year later: Cuban medical team draws on experience and partnerships. MEDICC Rev, 2011. 13(1): p. 52-5.
- Kirsch, T., L. Sauer, and D. Guha Sapir, Analysis of the international and US response to the Haiti earthquake: recommendations for change. Disaster Med Public Health Prep, 2012. 6(3): p. 200-8.
- Clarke, J.N., Transitional coordination in Sudan (2006-08): lessons from the United Nations Resident Coordinator's Office. Disasters, 2013. 37(3): p. 420-41.
- Zoraster, R.M., Barriers to disaster coordination: health sector coordination in Banda Aceh following the South Asia Tsunami. Prehosp Disaster Med, 2006. 21(1): p. s13-8.
- Pan Américan Health, O., Natural disasters: protecting the public's health. PAHO. Scientific Públication, (575): p. 119-119.
Leave a Comment
You must be logged in to post a comment.