
Pokémon Go is a new game that encourages players to venture outdoors and interact with others in the pursuit of virtual Pokémon characters. With more time spent outdoors overall and in sometimes large congregations, Pokémon Go players could inadvertently elevate their risk of exposure to mosquito-borne diseases when playing in certain areas at certain times of year. Here, we make an initial assessment of the possible scope of this concern in the continental United States, which experiences its highest seasonal transmission of West Nile, Zika, and other viruses during summer and early fall. In particular, we propose that the times of day when many disease-relevant mosquito species are most likely to engage in blood feeding coincide with times of day when Pokémon Go activity is likely to be high, and we note that locations serving as hubs of Pokémon Go activity may in some cases overlap with areas where these mosquitoes are actively engaged in blood feeding. Although the risk of mosquito-borne diseases in the continental U.S. is low overall and is unlikely to be impacted significantly by Pokémon Go, it is nonetheless important for Pokémon Go players and others who spend time outdoors engaging in activities such as barbecues and gardening to be aware of these ongoing risks and to take appropriate preventative measures in light of the potential for outdoor activity to modify individual-level risk of exposure. As Pokémon Go and other augmented reality games become available in other parts of the world, similar risks should be assessed in a manner that is consistent with the local epidemiology of mosquito-borne diseases in those areas.
Because of the potential link between the ongoing Zika virus outbreak and a surge in the number of cases of congenital microcephaly, officials in Latin America have recommended that women postpone pregnancy until this association is firmly established or the outbreak subsides. However, in all these countries a large proportion of babies are still born out of unplanned pregnancies. Teenage girls are particularly at high risk, as they often lack access to preventive contraception methods, or the knowledge to use them appropriately. To gauge the magnitude of the barriers preventing the implementation of such a recommendation in Brazil, the country so far most affected by the Zika epidemic, we evaluated pregnancy rates in teenage girls, and their spatial heterogeneity in the country, in recent years (2012-2014). Nearly 20% of children born in Brazil today (~560,000 live births) are by teenage mothers. Birth incidence is far higher in the tropical and poorer northern states. However, in absolute terms most births occur in the populous southeastern states, matching to a large extent the geographic distribution of dengue (an indicator of suitable climatic and sociodemographic conditions for the circulation of Aedes mosquitoes). These findings indicate that recommendation to delay pregnancy will leave over half a million pregnant adolescents in Brazil vulnerable to infection every year if not accompanied by effective education and real access to prevention.
Medical trainees face multiple barriers to participation in major outbreak responses such as that required for Ebola Virus Disease through 2014-2015 in West Africa. Hurdles include fear of contracting and importing the disease, residency requirements, scheduling conflicts, family obligations and lack of experience and maturity. We describe the successful four-week deployment to Liberia of a first year infectious diseases trainee through the mechanism of the Global Outbreak Alert and Response Network of the World Health Organization. The posting received prospective approval from the residency supervisory committees and employing hospital management and was designed with components fulfilling the Accreditation Council for Graduate Medical Education (ACGME) core competencies. It mirrored conventional training with regards to learning objectives, supervisory framework and assessment methods. Together with Centers for Disease Control and Prevention and many other partners, the team joined the infection prevention and control efforts in Monrovia. Contributions were made to a ‘ring fencing’ infection control approach that was being introduced, including enhancement of triage, training and providing supplies in high priority health-care facilities in the capital and border zones. In addition the fellow produced an electronic database that enabled monitoring infection control standards in health facilities. This successful elective posting illustrates that quality training can be achieved, even in the most challenging environments, with support from the pedagogic and sponsoring institutions. Such experiential learning opportunities benefit both the outbreak response and the trainee, and if scaled up would contribute towards building a global health emergency workforce. More should be done from residency accreditation bodies in facilitating postings in outbreak settings.
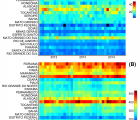
Chikungunya is an emerging arbovirus that is characterized into four lineages. One of these, the Asian genotype, has spread rapidly in the Americas after its introduction in the Saint Martin island in October 2013. Unexpectedly, a new lineage, the East-Central-South African genotype, was introduced from Angola in the end of May 2014 in Feira de Santana (FSA), the second largest city in Bahia state, Brazil, where over 5,500 cases have now been reported. Number weekly cases of clinically confirmed CHIKV in FSA were analysed alongside with urban district of residence of CHIKV cases reported between June 2014 and October collected from the municipality’s surveillance network. The number of cases per week from June 2014 until September 2015 reveals two distinct transmission waves. The first wave ignited in June and transmission ceased by December 2014. However, a second transmission wave started in January and peaked in May 2015, 8 months after the first wave peak, and this time in phase with Dengue virus and Zika virus transmission, which ceased when minimum temperature dropped to approximately 15°C. We find that shorter travelling times from the district where the outbreak first emerged to other urban districts of FSA were strongly associated with incidence in each district in 2014 (R2).
In the three West African countries most affected by the recent Ebola virus disease (EVD) outbreak, resistance to public health measures contributed to the startling speed and persistence of this epidemic in the region. But how do we explain this resistance, and how have people in these communities understood their actions? By comparing these recent events to historical precedents during Cholera outbreaks in Europe in the 19th century we show that these events have not been new to history or unique to Africa. Community resistance must be analysed in context and go beyond simple single-variable determinants. Knowledge and respect of the cultures and beliefs of the afflicted is essential for dealing with threatening disease outbreaks and their potential social violence.
Introduction: The eradication of a human infectious disease is a major challenge and, if achieved, represents a enormous achievement. This article explores the long and difficult journey towards eradication for polio and guinea worm.
Methods: The authors reviewed the programmatic approaches taken in the eradication strategies for these two diseases and the unique socio-political contexts in which these strategies are couched. The epidemiology of the last 15 years is compared and contrasted. The specific challenges for both programs are outlined and some key elements for success are highlighted.
Discussion: The success of these eradication programs is contingent upon many factors. Nothing is assured, and progress remains fragile and vulnerable to setbacks. Security must be ensured in guinea worm transmission areas in Africa and polio transmission areas in Pakistan and Afghanistan. Technical solutions alone cannot guarantee eradication. National leadership and continued international focus and support are necessary, today more than ever. The legacy of success would be extraordinary. It would reverberate to future generations in the same way that the eradication of smallpox does for this generation.
In this commentary, we consider the relationship between early outbreak changes in the observed reproductive number of Ebola in West Africa and various media reported interventions and aggravating events. We find that media reports of interventions that provided education, minimized contact, or strengthened healthcare were typically followed by sustained transmission reductions in both Sierra Leone and Liberia. Meanwhile, media reports of aggravating events generally preceded temporary transmission increases in both countries. Given these preliminary findings, we conclude that media reported events could potentially be incorporated into future epidemic modeling efforts to improve mid-outbreak case projections.
Vaccine hesitancy is often understood and explored on the level of individual decision-making. However, questions surrounding the risk and efficacy of vaccination are evident in wider public discourse; social narratives of vaccination inform and impact on the individual level. This paper takes a narrative analysis approach from the sociology of health to examine data drawn from a wider study on global public health responses to the H1N1 pandemic. The paper concentrates upon criticisms to mass vaccination as recounted within the Council of Europe’s debate of the handling of H1N1. It shows that three narratives were particularly dominant: problematizing the use of vaccination as a public health response; criticising the efficacy of the vaccines; and, questioning the safety of the strategy. This debate presents an important case study in understanding the way in which vaccines are problematized within the public discourse.
Today, according to many public health experts, public confidence in vaccines is waning. The term “vaccine hesitancy” (VH) is increasingly used to describe the spread of such vaccine reluctance. But VH is an ambiguous notion and its theoretical background appears uncertain. To clarify this concept, we first review the current definitions of VH in the public health literature and examine its most prominent characteristics. VH has been defined as a set of beliefs, attitudes, or behaviours, or some combination of them, shared by a large and heterogeneous portion of the population and including people who exhibit reluctant conformism (they may either decline a vaccine, delay it or accept it despite their doubts) and vaccine-specific behaviours. Secondly, we underline some of the ambiguities of this notion and argue that it is more a catchall category than a real concept. We also call into question the usefulness of understanding VH as an intermediate position along a continuum ranging from anti-vaccine to pro-vaccine attitudes, and we discuss its qualification as a belief, attitude or behaviour. Thirdly, we propose a theoretical framework, based on previous literature and taking into account some major structural features of contemporary societies, that considers VH as a kind of decision-making process that depends on people’s level of commitment to healthism/risk culture and on their level of confidence in the health authorities and mainstream medicine.
An unprecedented epidemic of Zaire ebolavirus (EBOV) has affected West Africa since approximately December 2013, with intense transmission on-going in Guinea, Sierra Leone and Liberia and increasingly important international repercussions. Mathematical models are proving instrumental to forecast the expected number of infections and deaths and quantify the intensity of interventions required to control transmission; however, calibrating mechanistic transmission models to an on-going outbreak is a challenging task owing to limited availability of epidemiological data and rapidly changing interventions. Here we project the trajectory of the EBOV epidemic in Liberia by fitting logistic growth models to the cumulative number of cases. Our model predictions align well with the latest epidemiological reports available as of October 23, and indicates that the exponential growth phase is over in Liberia, with an expected final attack rate of ~0.1-0.12%. Our results indicate that simple phenomenological models can provide complementary insights into the dynamics of an outbreak and capture early signs of changes in population behavior and interventions. In particular, our results underscore the need to treat the effective size of the susceptible population as a dynamic variable rather than a fixed quantity, due to reactive changes in transmission throughout the outbreak. We show that predictions from the logistic model are more variable in the earlier stages of an epidemic (such as the EBOV epidemics in Sierra Leone and Guinea). More research is warranted to compare the performances of mechanistic and phenomenological approaches for disease forecasts, before such predictions can be fully used by public health authorities.
Commentary The ongoing Ebola outbreak is taking place in one of the most highly connected and densely populated regions of Africa (Figure 1A). Accurate information on population movements is valuable for monitoring the progression of the outbreak and predicting its future spread, facilitating the prioritization of interventions and designing surveillance and containment strategies. Vital questions […]